The Delta Dispatch

CFD Application Guide for Aspiring Firefighters
Dreaming of becoming a Calgary firefighter? This guide walks you through the CFD application process, including essential certifications, physical fitness tips, suggested courses, and how Delta Emergency Support Training can help you succeed.
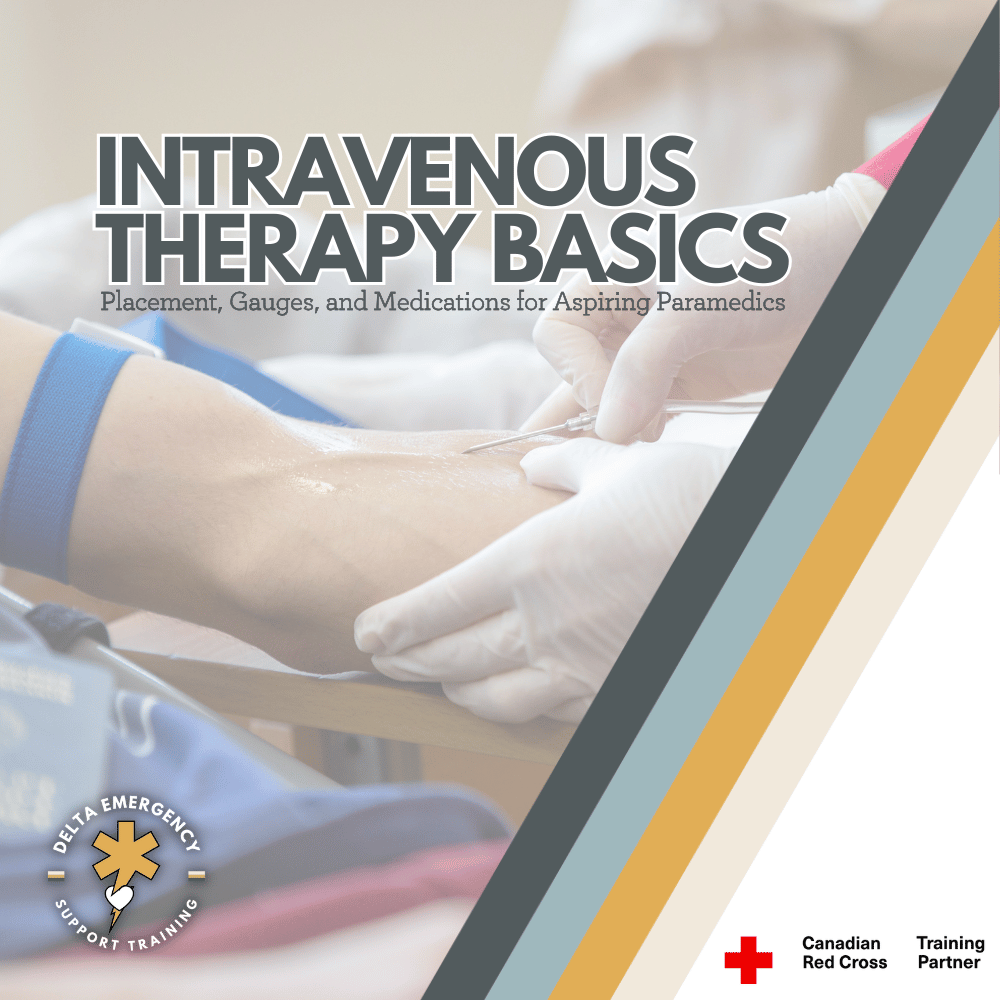
Intravenous Therapy for Beginners: Placement, Gauges & Medications
Intravenous (IV) therapy is a key skill for future paramedics and advanced responders. This beginner’s guide covers vein selection, catheter sizes, and common medications, helping you prepare for PCP training and real-world prehospital care.

From the Rigs to the Fire Hall: Get Your Advanced First Aid Certification in 2026
Thinking about leaving the rigs to pursue firefighting? Our Camp Rotation Advanced First Aid courses for 2026 are designed for rig workers with demanding schedules. Get certified, gain real-world emergency skills, and take the first step toward a career saving lives.

Rate, Rhythm, and Quality: How to Assess Pulse and Breathing in the Field
Assessing rate, rhythm, and quality of pulse and respirations is essential for identifying serious patient conditions. Learn how to conduct these key evaluations in the field with accuracy.

Ejection Trauma: What First Responders Need to Know About High-Impact MVCs
Ejection trauma is one of the most catastrophic outcomes of a motor vehicle collision. For first responders, understanding how to assess, stabilize, and prioritize care for these high-impact patients is critical. Here’s how to stay calm, organized, and effective in the moments that matter most.

Traumatic Cardiac Arrest: What Every Professional Responder Should Know
Traumatic cardiac arrest is one of the most demanding situations a responder can face. This in-depth guide explains how to rapidly identify reversible causes, manage airway and bleeding, and provide effective field care to improve survival chances in severe trauma cases.

Treating Gunshot Wounds: A Professional Responder’s Guide
Gunshot wounds are life-threatening emergencies that require quick, precise action. This guide for professional responders covers wound assessment, bleeding control, chest seal application for thoracic injuries, and key steps for safe transport to trauma centers.

Suspected Pelvic Fractures: A Guide for Advanced First Aiders
Pelvic fractures are serious injuries that can lead to life-threatening internal bleeding. This guide for advanced first aiders covers common causes such as vehicle collisions and falls from height, how to recognize signs and symptoms in the field, and step-by-step instructions for proper pelvic immobilization, including correct binder placement over the iliac crests. Learn how to provide effective prehospital care while minimizing complications and preparing for rapid transport.

Understanding Basic, Intermediate, and Advanced Airway Adjuncts in Prehospital Care
Airway management is the cornerstone of emergency care. From simple oropharyngeal and nasopharyngeal airways to supraglottic devices and endotracheal intubation, prehospital providers need to know when—and how—to use each tool. This guide explains the essential skills and decision-making strategies for basic, intermediate, and advanced airway adjuncts to help responders keep patients breathing and safe.

Hypoxia 101: Symptoms, Causes, and First Aid Tips
Hypoxia can lead to irreversible brain damage within minutes. Rapid recognition, airway management, aggressive oxygenation, and swift treatment of the underlying cause—especially opioid-related respiratory depression—are essential to preserving neurological function and improving outcomes.
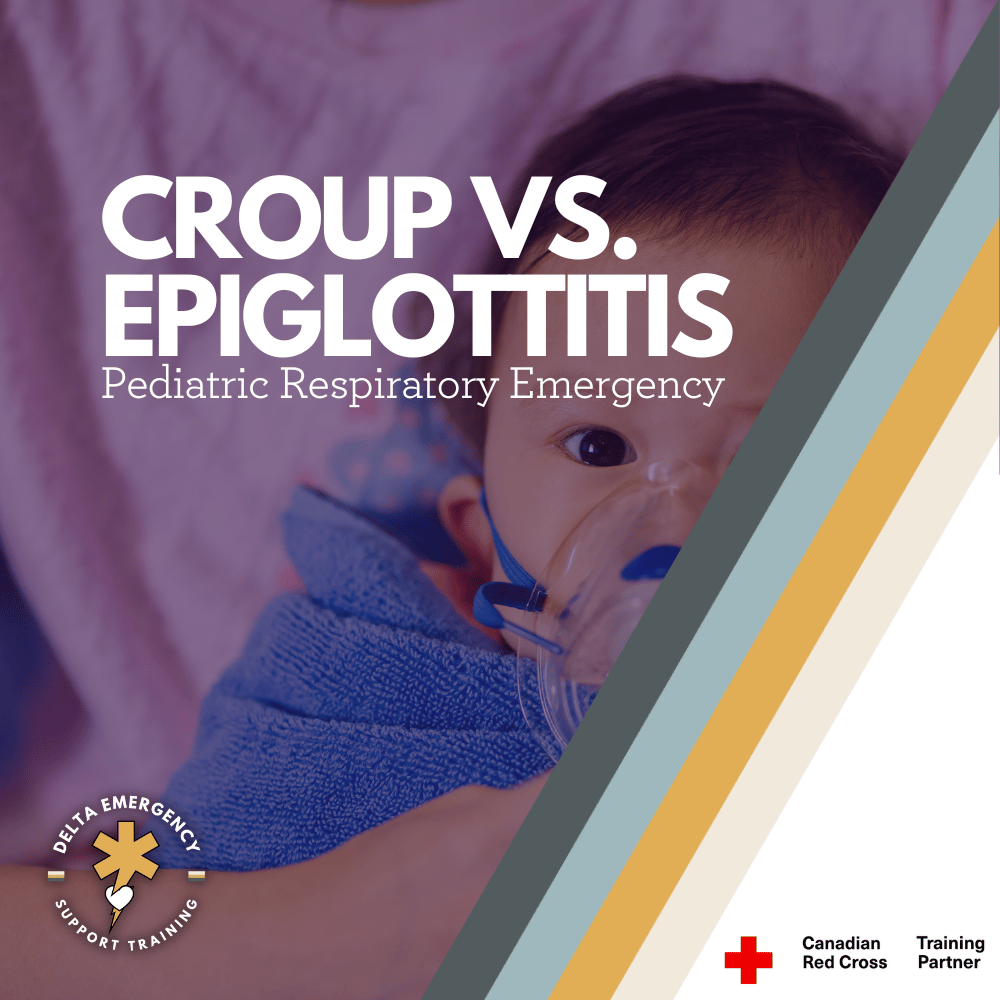
Croup vs. Epiglottitis in Children: What First Responders and Parents Need to Know
Breathing problems in children can be terrifying, and knowing the difference between croup and epiglottitis could save a life. Parents need to know the warning signs, while first responders must act quickly and carefully. Here’s how to tell them apart and what steps to take in an emergency.

Distracting Injuries: Pulling Focus and Masking Pain
In trauma care, some injuries grab all the attention—but they aren’t always the deadliest. Distracting injuries can mislead responders and mask life-threatening conditions. Here’s what every first responder needs to know about spotting them, staying systematic, and keeping patient safety the top priority.

Becoming a Paramedic in Canada: How EMR Training Fits Into the Bigger Picture
Thinking about becoming a paramedic in Canada? It starts with understanding the paramedicine pathway. This blog explains where EMR training fits into the journey and why it’s a key first step toward a rewarding career in emergency services.

Alberta Fire Applicants & EMRs: Master the Medical Portion with Paramedics and Firefighters
Succeeding in the medical portion of a firefighter or EMR application in Alberta comes down to mastering the fundamentals under pressure. At Delta Emergency Support Training, active paramedics and firefighters teach you vital patient assessment skills, accurate vitals, effective communication, and safe medication administration.

Pulmonary Embolism for EMR Students: Signs, Symptoms, and Action Steps
Pulmonary embolisms are among the most serious complications post-surgery—and often go unnoticed until it’s too late. For Emergency Medical Responders, especially those working in Alberta’s high-risk environments, knowing the subtle signs and acting fast can make all the difference. This blog breaks down what to look for, how to respond, and why early recognition matters.

Your Mental Checklist for Altered Level of Consciousness Calls
Altered level of consciousness (LOC) can signal everything from trauma to stroke, overdose, or diabetic emergencies. For EMRs and Advanced First Aiders, quick assessment using tools like AVPU and GCS is essential. Learn how to approach LOC calls with confidence and clinical clarity.

From Oilfield to Firehall: Why Tradespeople Are Switching to Emergency Services
Many tradespeople in Alberta’s oil and gas sector are transitioning to emergency services careers. At Delta Emergency Support Training in Calgary, our Advanced First Aid course provides the essential skills and certification needed to make that move with confidence.
Planning to Apply to Edmonton or Calgary Fire? Why Advanced First Aid Recertification Matters
Planning to apply to Calgary or Edmonton Fire? Delta Emergency Support Training in Calgary offers Advanced First Aid recertification taught by paramedics and firefighters. Choose from weekday or weekend formats between September and November. Build your resume and keep your skills current with this Red Cross-certified course.