The Delta Dispatch

Why First Responders Use Vital Signs: A comprehensive guide
Vital signs are measurements of the body's basic functions and are used to assess a person's overall health and wellbeing. There are four primary vital signs: body temperature, pulse rate, blood pressure, and respiratory rate. Each vital sign provides important information about a person's health and can help identify underlying health conditions or other problems.
Body temperature is a measure of the body's internal heat and is typically measured using a thermometer. A fever is generally defined as a body temperature above 100.4°F (38°C) and can indicate an infection or other underlying health condition.
Pulse rate is a measure of the heart rate, or the number of times the heart beats per minute. A rapid pulse may indicate a fever, dehydration, or an irregular heartbeat, while a slow pulse may indicate heart disease or other health conditions.
Blood pressure is a measure of the force of blood against the walls of arteries as the heart pumps blood through the body. High blood pressure, or hypertension, can increase the risk of heart disease, stroke, and other health problems.
Respiratory rate is a measure of the number of breaths a person takes per minute. A rapid respiratory rate may indicate an underlying health condition, such as asthma or pneumonia.
Monitoring vital signs is an essential part of healthcare and can help healthcare professionals and first responders make informed decisions about treatment and care.
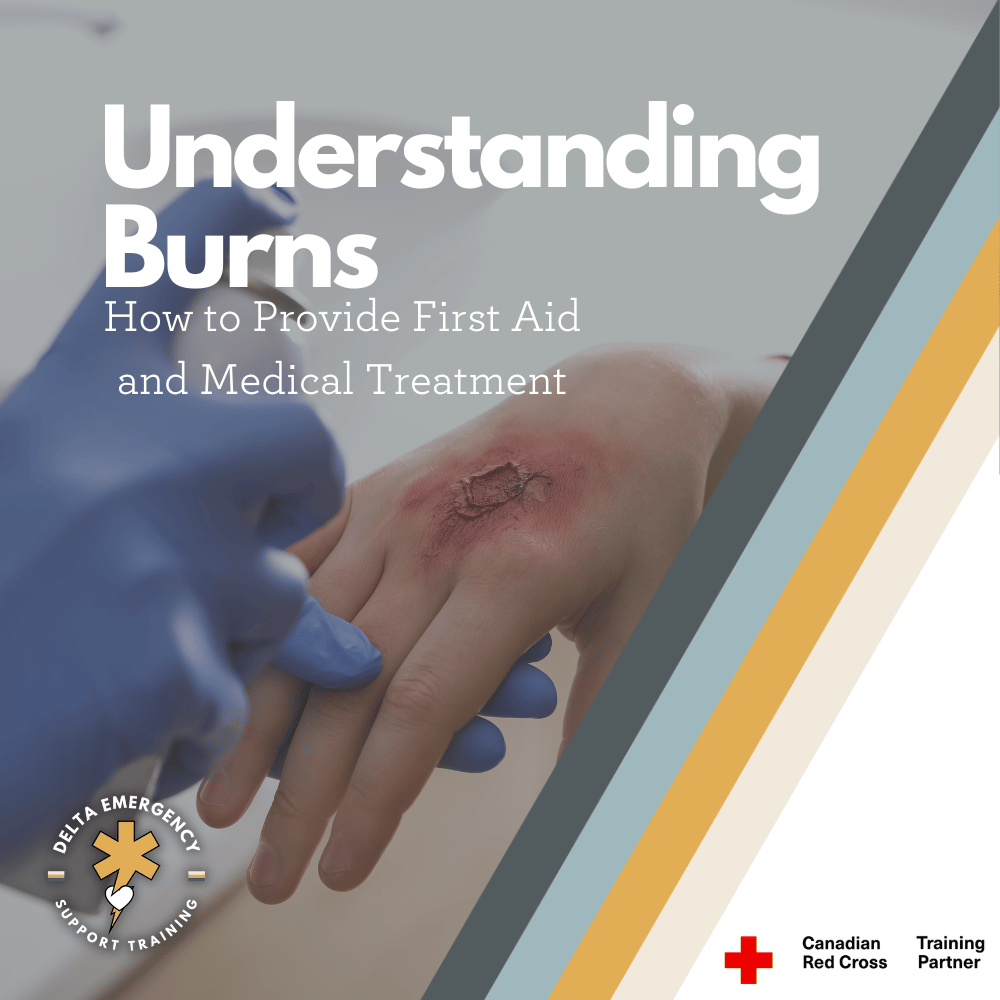
Burn Management: Understanding Burns and How to Provide First Aid
Depending on the severity of the burn, it can be a painful and potentially life-threatening injury. Superficial burns only affect the outer layer of skin and typically result in redness, pain, and mild swelling. Partial-thickness burns affect both the outer and underlying layer of skin and can result in blisters, severe pain, and swelling. Full-thickness burns are the most severe type of burn, affecting all layers of skin and potentially even deeper tissue. Full-thickness burns can result in blackened or charred skin and can cause nerve damage, muscle and bone damage, and even death.
If you or someone else experiences a burn, providing first aid as soon as possible is crucial for promoting healing and preventing complications. The first step is to remove the source of the burn, such as a hot object or a chemical. Then, run cool (not cold) water over the burned area for at least 10-20 minutes. After that, cover the burn with a sterile, non-adhesive bandage or cloth. If the burn is severe, seek medical attention immediately.
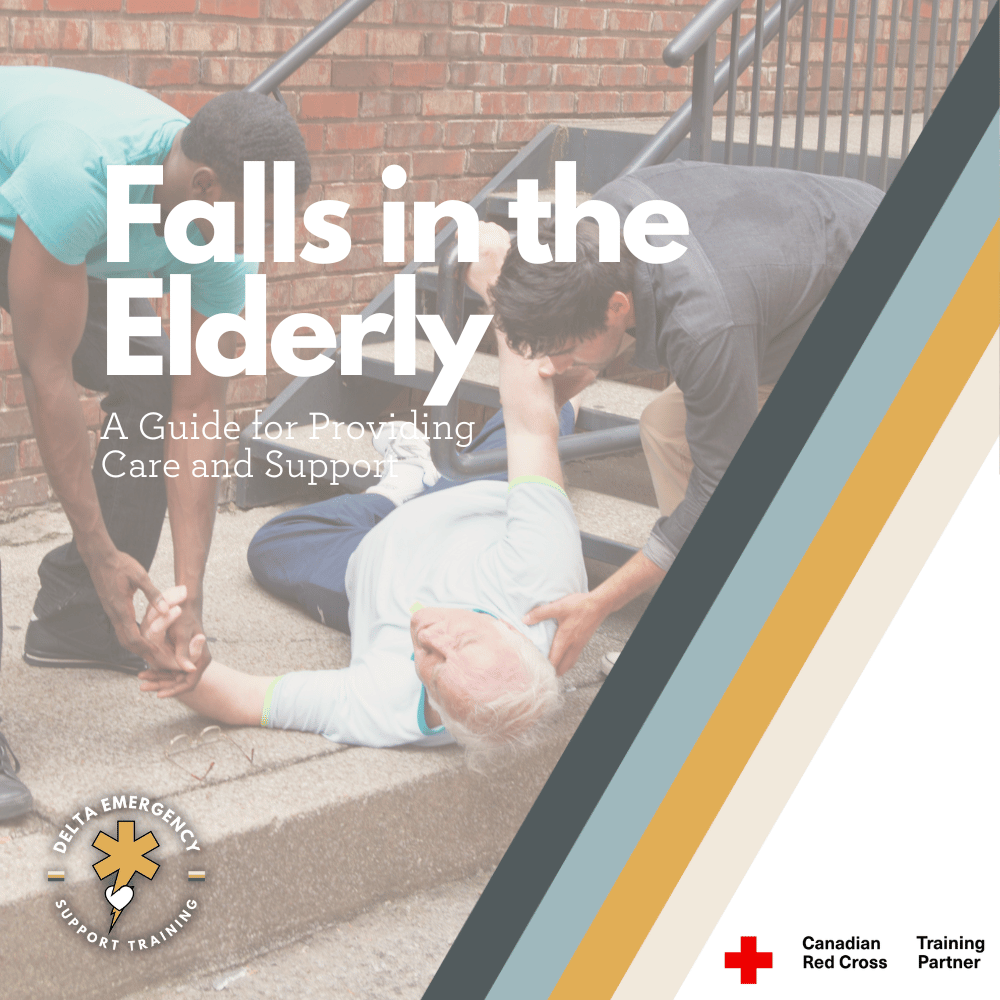
Assisting Elderly Who Have Fallen: A Comprehensive Guide to Providing Care and Support
Encountering an elderly or geriatric person who has fallen can be a difficult and distressing experience. Falls are a common problem among older adults and can lead to serious injuries, such as broken bones, head trauma, and bruises. It's important to approach the situation with care and sensitivity and take steps to provide appropriate assistance. Whether you're a family member, caregiver, or passerby, knowing what to do when you find an injured elderly person who has fallen can help to ensure their safety and well-being. In this blog post, we'll explore some general steps you can take to provide valuable assistance and help to ensure that the person receives the care and treatment they need.

Responding to Mass Casualty Incidents: A Guide for First Responders
Responding to Mass Casualty Incidents is a critical aspect of emergency preparedness and response. Whether it's a natural disaster, a terrorist attack, or an accident, the ability to quickly and effectively manage large numbers of injured victims can mean the difference between life and death. In such situations, emergency responders must work together to triage, treat, and transport the injured to medical facilities. They must also ensure that the scene is secure and that all necessary resources are available to address the needs of those affected.

Emergency Transport How to Package a Patient Outdoors
Packaging a patient outdoors involves preparing the patient for transport while outside of a hospital or medical facility. This can be necessary if the patient is injured in a remote location, such as a hiking trail, or if the patient needs to be moved quickly due to a hazardous environment, such as a chemical spill. The process of packaging a patient outdoors requires careful planning and execution by trained emergency responders.
Once the situation has been assessed, the responders must stabilize the patient's injuries. This may involve applying pressure to a wound, immobilizing a broken bone, or providing oxygen to a patient who is having difficulty breathing. The goal is to ensure that the patient is as comfortable and stable as possible before transport.
Depending on the patient's injuries and the environment, there are several different methods for packaging a patient outdoors. Some of the most common methods include a vacuum mattress, a scoop stretcher, or a portable stretcher. The chosen method should be able to support the patient's weight and immobilize any injured limbs or body parts.

Unraveling the Mystery of the Heart's Electrical Dance: How Your Heart Beats to Its Own Rhythm!
Heart's Electrical Conduction - Key Concepts and Terminology. Delve into the intricacies of the heart's electrical conduction system with our comprehensive overview. Learn about the physiology, function, and regulation of the heart's electrical pathways. Gain a deeper understanding of this vital organ's complex conduction system with our informative blog.

On the Frontline: Mastering Scene Assessment for AFA with Calgary & Edmonton Fire Departments
During an emergency, AFAs are trained to conduct thorough scene assessments to gather crucial information that informs the appropriate course of action. This includes assessing the safety of the scene, identifying hazards, evaluating the mechanism of injury or nature of illness, and determining the number of patients and their condition. By working closely with Calgary & Edmonton Fire Departments, we (EMS) can collaborate on scene management strategies, coordinate resources, and prioritize patient care based on the severity of injuries or illnesses.

What is an EMR?
The first step for an EMR is to assess the situation for hazards that can harm themselves, their partners, and their patients, and determine the nature of the emergency. They need to determine the level of medical attention needed and make quick decisions…

SMR - Spinal Motion Restriction | Professional Responder Skill Series
While SMR is generally considered a safe and effective method for preventing spinal cord injury, there are certain risks and considerations that must be taken into account, such as the potential…

Calgary and Edmonton Fire Applications Opening in 2022 and 2023!
So you meet the minimum requirements to apply for Calgary and Edmonton Fire. What certifications do you need before you’re given a job offer? Canadian Red Cross Advanced First Aid is one of the certification requirements, and at Delta Emergency, we fully certify you to Alberta Fire Department standards.

Delta Emergency Hybrid Red Cross Advanced First Aid
We started teaching this new version of Hybrid Advanced First Aid in June 2021. Every student has rated our program with 5 stars and they all recommend it to their peers. 60 hours of at home learning and 24 hours in-class over 1 Friday night, Saturday and Sunday. Certify as an Advanced First Aider through online content such as videos, skill sheets, quizzes, written group discussions, 1:1 video instructor video sessions, weekly workbooks - more than multiple choice questions, games and repeatable tests to test your comprehension. Real instructors with real emergency experience. Skill sessions that deliver quality scenarios. Group scenarios to develop real world teamwork.